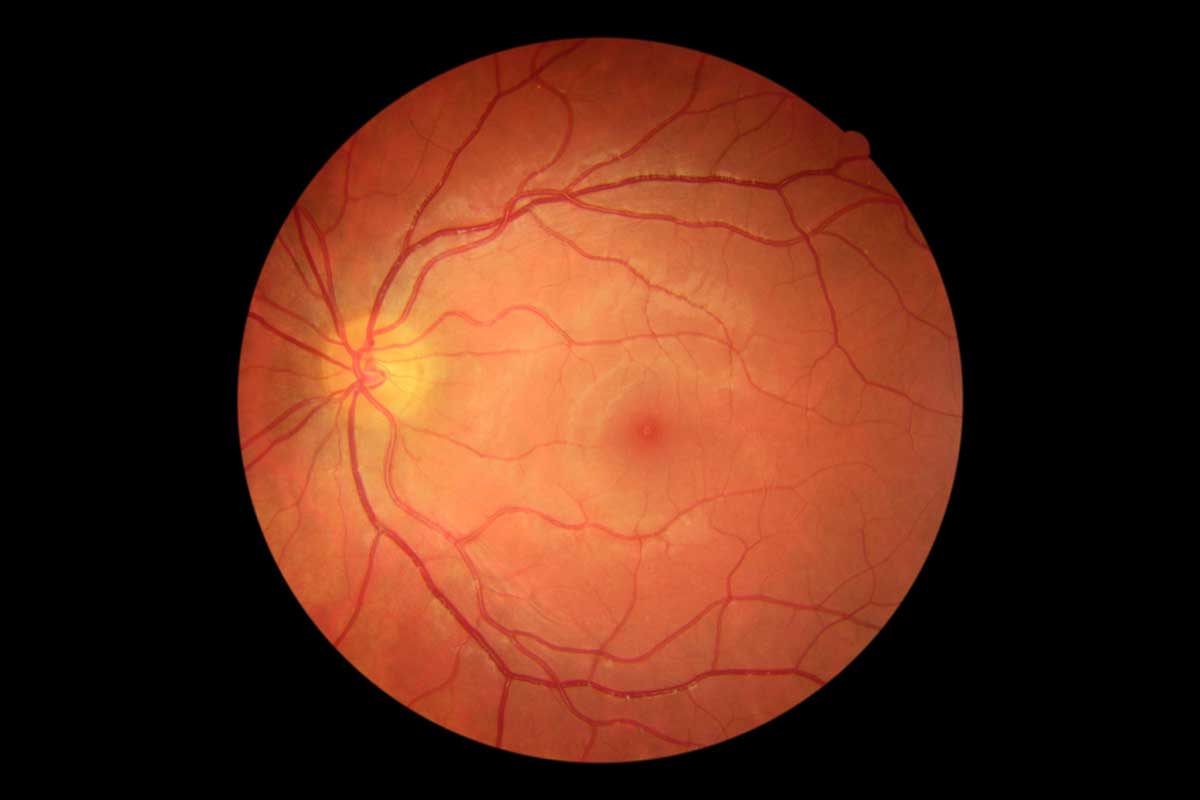
Diabetic retinopathy (DR) is a complication of diabetes mellitus (DM) and is an important cause of avoidable blindness worldwide. Over time, diabetes causes damage to many organs in your body, including the retina. Your retina helps you see by acting as the film projector in the back of your eye, projecting the image to your brain.
Diabetes damages the tiny blood vessels that nourish the retina. In the early stages, known as non-proliferative or background retinopathy, the vessels in the retina weaken and begin to leak, forming small, multiple dots of bleeding. When retinopathy advances, the decreased blood circulation deprives the retina of oxygen resulting in a condition called Diabetic Retinopathy.
Watch a video on diabetic retinopathy
Diabetic retinopathy can lead to severe visual loss or blindness in 2 ways. The first is when it affects your macula, the central part of your retina that provides you with sharp, central vision. When this part becomes swollen, it is called diabetic maculopathy. At the same time, blood vessels can also become blocked or closed, and parts of the retina die. New, abnormal, blood vessels may then start to grow along the retina and surface of the vitreous (the transparent gel that fills the inner part of the eye).
BMJ photo of Diabetic Maculopathy
Unfortunately, these delicate vessels can bleed easily. Blood may leak into the retina and vitreous, causing “floaters” (spots that appear to drift in front of the eyes), along with a decreased vision. This is called proliferative diabetic retinopathy, and it can even cause scar tissue which can pull off the retina, causing what’s called a tractional retinal detachment (TRD). In the later phases of the disease, continued abnormal vessel growth and scar tissue may cause a total retinal detachment and glaucoma. The result of either problem, if left untreated, is loss of sight and potentially blindness.
Symptoms of Diabetic Retinopathy
You may not be aware of the symptoms of DR in the initial stages of the condition unless it progresses quickly to the more severe stages. The symptoms of DR include:
• Blurred vision • Sudden loss of vision in one eye • Seeing rings around lights • Dark spots or flashing lights
The symptoms described above may not necessarily mean that you have diabetic retinopathy. However, if you experience one or more of these symptoms, do consult your ophthalmologist for a comprehensive eye examination. The following are the risk factors which can increase the risk or accelerate Diabetic Retinopathy ;
A dilated retinal examination will be recommended by your ophthalmologist to examine the retina and detect the presence of any diabetic changes in the eye.
In addition to this, your ophthalmologist may also recommend certain diagnostic procedures such as a fundus fluorescein angiogram (FFA) or optical coherence tomography (OCT) to assess the severity of DR and to determine the best mode of treatment. The angiogram test involves the injection of fluorescein (a yellow dye) into your arm. The dye can then be seen coursing through the blood vessels in your retina and photos are taken. Normal, healthy blood vessels do not leak, however, damaged blood vessels like in DR do, thus helping to target treatment. An OCT retina scan uses reflected light to build a cross-sectional image of the retina. Macular oedema is noted when areas of your retina are shown to contain spaces filled with fluid (see below).
In mild cases, treatment may not be necessary. Regular eye exams are important for monitoring the progression of the disease. Strict control of blood sugar and blood pressure levels can greatly reduce or prevent DR. In more advanced cases, treatment may be recommended by your Eye Specialist to stop the damage of DR, to prevent vision loss and to potentially restore vision.
How To Reduce the Risk of Diabetic Retinopathy
Visit your ophthalmologist or optometrist at least once a year. You may be recommended to visit more or less frequently depending on your situation.
Know your HbA1c (a test of your average blood glucose level over three months). Most people with diabetes should aim for a target of lower than 7%. Talk to your healthcare team about what your target should be.
View NIH video on Diabetic Eye Examination
Who Should have their Eyes Examined by an Eye Specialist
All individuals with either Type I or Type II diabetes should be screened annually.
The interval for follow-up assessments should be tailored according to the severity of the retinopathy. In those with no or minimal retinopathy, the recommended interval is one to two years.
Women with type I or type II diabetes or women has diabetic risk and plan to become pregnant should be screened before conception, during the first trimester, as needed during pregnancy and within the first year postpartum.
Check your vision regularly (at least once a month) using Amsler Grid and Vision Chart to monitor your eye condition (especially if you are at risk of developing Diabetic Retinopathy)
Disclaimer. TELEME blog posts contains general information about health conditions and treatments. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. The information is not advice and should not be treated as such.
If you think you may be suffering from any medical condition, you should seek immediate medical attention from your doctor or other professional healthcare providers. You should never delay seeking medical advice, disregard medical advice, or discontinue medical treatment because of information on this website.
How useful was this post?
Click on a star to rate it!
Average rating / 5. Vote count:
No votes so far! Be the first to rate this post.
As you found this post useful...
Share it on social media!
We are sorry that this post was not useful for you!
Let us improve this post!
Tell us how we can improve this post?
You May Like This
Pre-Diabetes / Diabetic Risk Pre-Diabetes / Diabetic Risk Diabetes are caused by a combination of the risk factors listed…