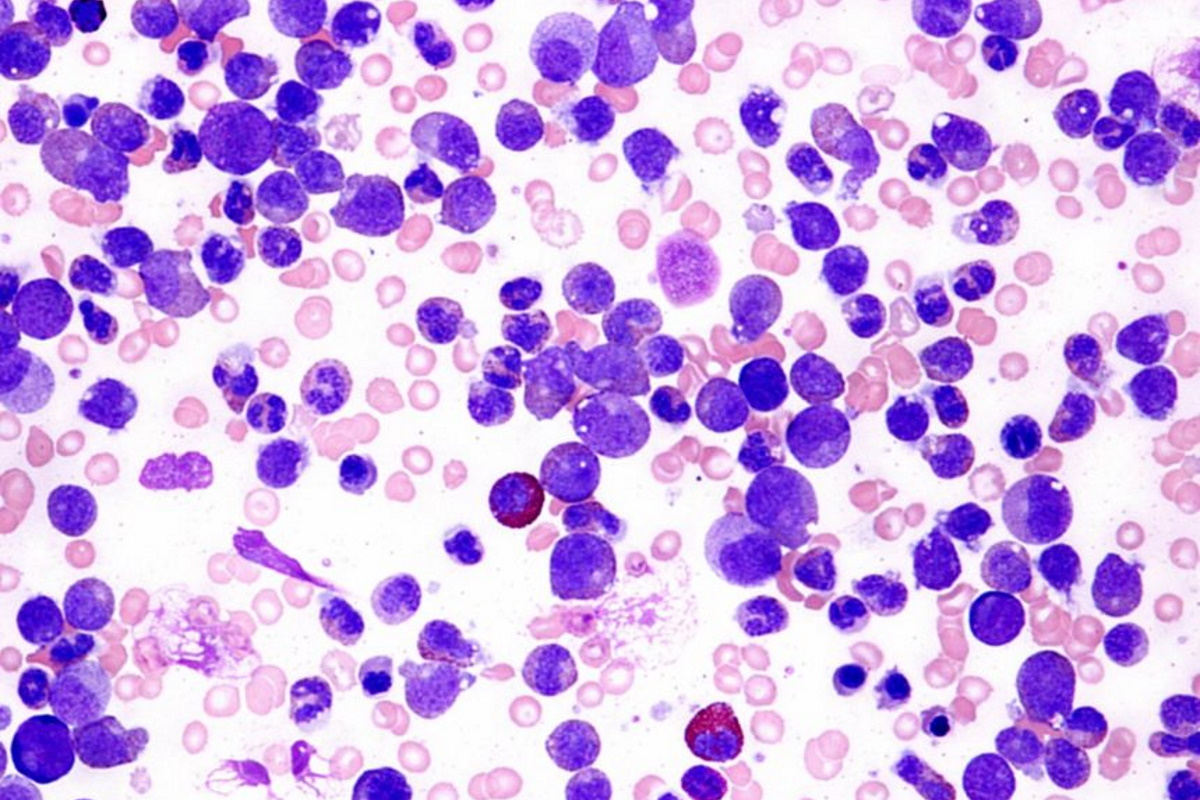
The bone marrow normally makes blood stem cells that become mature blood cells such as red blood cells, white blood cells (also known as granulocytes) and platelets over time. These cells play a vital role in keeping our body healthy by carrying oxygen, fighting infections and helping blood to clot). Chronic Myeloid Leukaemia (CML) is a cancer of the white blood cells where there is an increased and uncontrolled production of myeloid cells in the bone marrow resulting in abnormal immature blood cells (also known as blast cells) which do not function normally. Due to the uncontrolled growth of these blast cells, the red blood cells and platelets production are reduced resulting in anaemia and possible bleeding tendency.
CML accounts for 15–25% of all adult leukemias. CML can be classified into 3 phases based on test results and clinical signs.
Chronic phase (usually over 85% of CML cases are in the chronic phase)
Accelerated phase (where there is persistently high white blood cells with low red blood cells and platelets. There is less than 19% blasts in the blood or bone marrow)
Blast crisis (where there is >20% blasts in the blood or bone marrow and is considered to be acute leukemia)
Click to view CancerGPS video on CML
Cause
The cause is attributed to the presence of a specific acquired (not inherited) genetic defect called Philadelphia chromosome which can be found in almost all patients. The cause of CML is unknown although exposure to toxins such as benzene or excessive radiation may be a risk factor.
Signs and Symptoms
Majority of patients are asymptomatic. Some of the symptoms include;
Fever and night sweats
Spleen enlargement with discomfort and pain
Loss of appetite
Early satiety (feel full quite quickly)
Unexplained weight loss
Bleeds or bruise easily
Diagnosis and Tests
Blood tests shows increased number of granulocytes of all types including neutrophils, basophils and eosinophils
Genetic testing to look for the presence of Philadelphia chromosome by cytogenetic study or presence of BCR-ABL gene by PCR test
Treatment
Treatment of CML with Tyrosine Kinase Inhibitors (TKI) medication works by inhibiting the growth of these leukemias cells and promoting cell death, thus preventing disease progression sufficiently to achieve regrowth of their normal bone marrow stem cell population so that these myeloid cells can mature into normal white blood cells. This will be reflected by complete cytogenetic response and major or molecular response (with the disappearance of the abnormal gene).
Imatinib mesylate (known as Gleevec or Glivec)
Dasatinib (Sprycel)
Nilotinib (Tasigna)
Ponatinib (Iclusig)
Asciminib (Scemblix)
Patients may develop some resistance with time, but doctors have several types of TKI medications to choose from. Patients need regular check ups every 3-6 months to monitor their blood counts and genetic response.
Prognosis
In the past, the median survival time for CML patients was only around 3–5 years but the use of tyrosine kinase inhibitors has improved overall survival rates dramatically to over 95% which is as good as a medical cure. Follow up and regular testing by your Specialist is essential to ensure successful outcomes.
Discuss the test results and treatment plan with your haematologist
Disclaimer. TELEME blog posts contains general information about health conditions and treatments. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. The information is not advice and should not be treated as such.
If you think you may be suffering from any medical condition, you should seek immediate medical attention from your doctor or other professional healthcare providers. You should never delay seeking medical advice, disregard medical advice, or discontinue medical treatment because of information on this website.
How useful was this post?
Click on a star to rate it!
Average rating / 5. Vote count:
No votes so far! Be the first to rate this post.
As you found this post useful...
Share it on social media!
We are sorry that this post was not useful for you!
Let us improve this post!
Tell us how we can improve this post?
You May Like This
CAR T-Cell (CART) Therapy CAR T-Cell Therapy (CART) Chimeric Antigen Receptor T-cell therapy (also known as CAR-T therapy) is…

 Therapy")
")



